For years, the standard clinical advice for a damaged tendon was effectively this: manage the pain, build strength in the surrounding muscle, and accept that the tissue itself probably wouldn’t change.
The reasoning seemed scientifically sound. Tendons have a significantly lower blood supply than muscle — especially in their core, the region where most tendinopathy develops. Without adequate circulation, meaningful cellular repair seemed unlikely. The collagen matrix of a damaged tendon was treated as largely fixed. You could compensate around it. You couldn’t fix it.
That view is now obsolete.
A body of research over the past two decades has demonstrated something that genuinely surprised the rehabilitation world: damaged tendon tissue can remodel. Not just reduce in pain — actually rebuild structurally, with new collagen reorganised into stronger, denser fibre arrangements. And it does so in response to a specific type of mechanical loading that most people in gyms have never used.
Understanding that loading is what this article is about.
Why Tendons Are Different From Muscle
Most people who train consistently understand — at least intuitively — how muscle grows. Load it, create tension, recover, repeat. The tissue adapts visibly and relatively quickly.
Tendons don’t operate the same way.
Their collagen turns over slowly. Blood supply is limited, particularly in the mid-substance — the region that’s most often damaged in patellar and Achilles tendinopathy. And critically, tendons don’t respond to the same mechanical signals that build muscle. High-speed, explosive movement creates an enormous demand on muscle. For the tendon, particularly in areas of existing damage, fast loading often bypasses the tissue entirely.
This is the mechanism of stress shielding. When a tendon has to lengthen rapidly — as during a jump, a sprint, or a heavy Olympic pull — the healthy surrounding tissue absorbs most of the force to protect the disrupted region. The damaged area gets shielded. It never receives the stimulus it needs to actually remodel.
This is why people with patellar tendinopathy often feel fine during slow training but flare immediately on plyometrics. And it’s why rest followed by a return to sport tends to be a temporary fix. The tissue was never addressed — just the irritation.
The practical consequence: you can train seriously for years, build substantial muscle, and still have tendons that have never meaningfully adapted to any specific loading stimulus. Tendons are chronically undertrained in most fitness programmes, not because of effort, but because no one is applying the right stimulus to them.
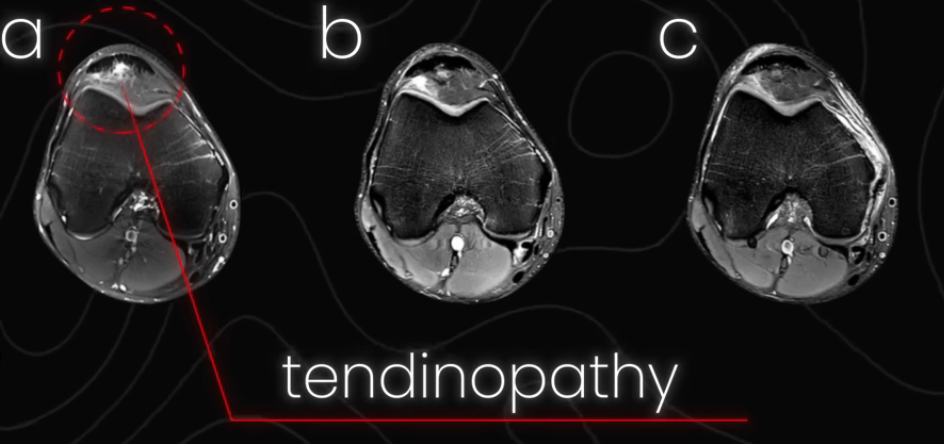
MRI cross-sections of an NBA athlete’s patellar tendon. Left: image a shows active tendinopathy — the disrupted, irregular area circled in red at the top of the scan. Right: the same tendon at six and eighteen months of targeted loading. The damaged tissue has been replaced by organised, structurally healthy collagen.
What the Research Shows
The MRI sequence above was, for a long time, considered an implausible outcome. The assumption in sports medicine was that once tendon tissue was disrupted to that degree, the structural changes were largely permanent. You could work around it. You couldn’t undo it.
The 18-month timeline shown here was already significant. But it’s not the floor of what’s possible.
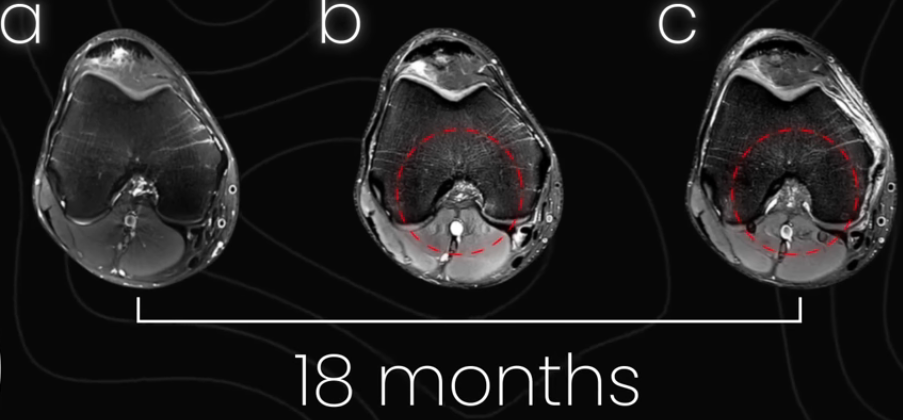
A sagittal (side-view) MRI of the same tendon from a different angle. The left image shows a thin, structurally compromised tendon. The right image shows the same structure after 18 months — substantially thicker and denser. The tissue has not only healed but grown.
More recent cases have documented tendon remodeling in considerably shorter windows — months rather than a year and a half — in athletes who loaded with appropriate intensity and consistency.
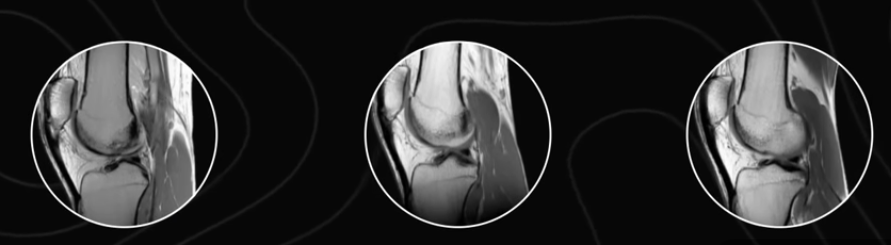
Ultrasound imaging of a competitive athlete’s tendon. Left: a disrupted, damaged structure. Right: the same tendon in under two months of targeted loading — visibly thicker, more organised, and structurally stronger.
The difference between an 18-month timeline and a two-month one isn’t genetics. It comes down to three specific variables in how the loading was applied.
The Three Variables: Time, Tension, Volume
The mechanism that drives tendon remodeling is called stress relaxation. Here is what that means in practical terms.
When you hold a static muscle contraction — an isometric — the muscle slowly shortens while the tendon slowly lengthens under maintained load. That gradual, controlled lengthening is the mechanical event that reaches the damaged tissue and signals the collagen matrix to reorganise. It bypasses the stress shielding that fast loading creates, because the lengthening is slow enough that the healthy tissue around the damaged region cannot fully protect it.
This is why isometric exercises — a split squat hold, a leg extension hold, a calf raise hold — are the primary tool for tendon adaptation. Not stretching. Not light pain-free range of motion. Heavy, sustained, static contractions.
Three variables determine whether those isometrics actually produce structural change.
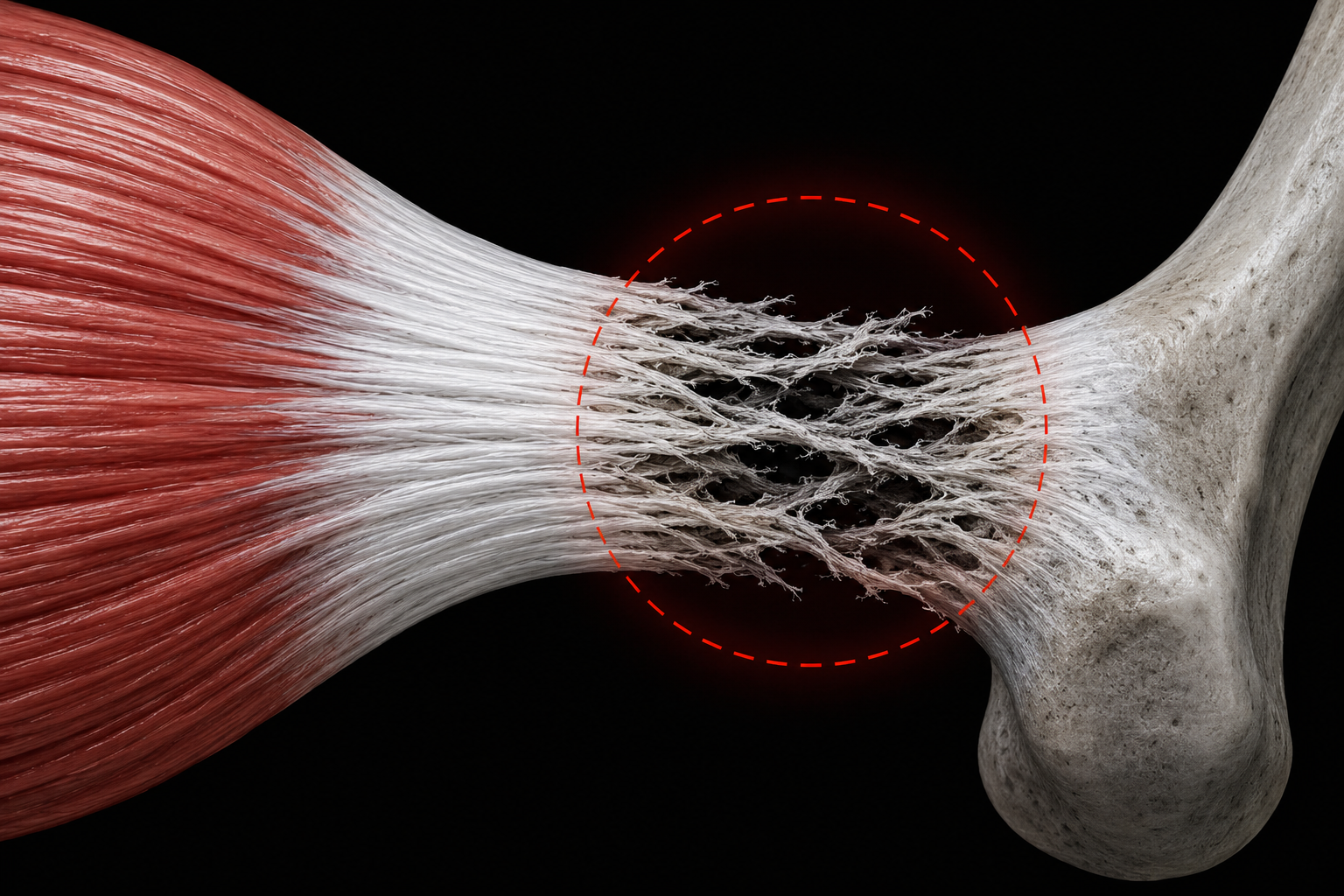
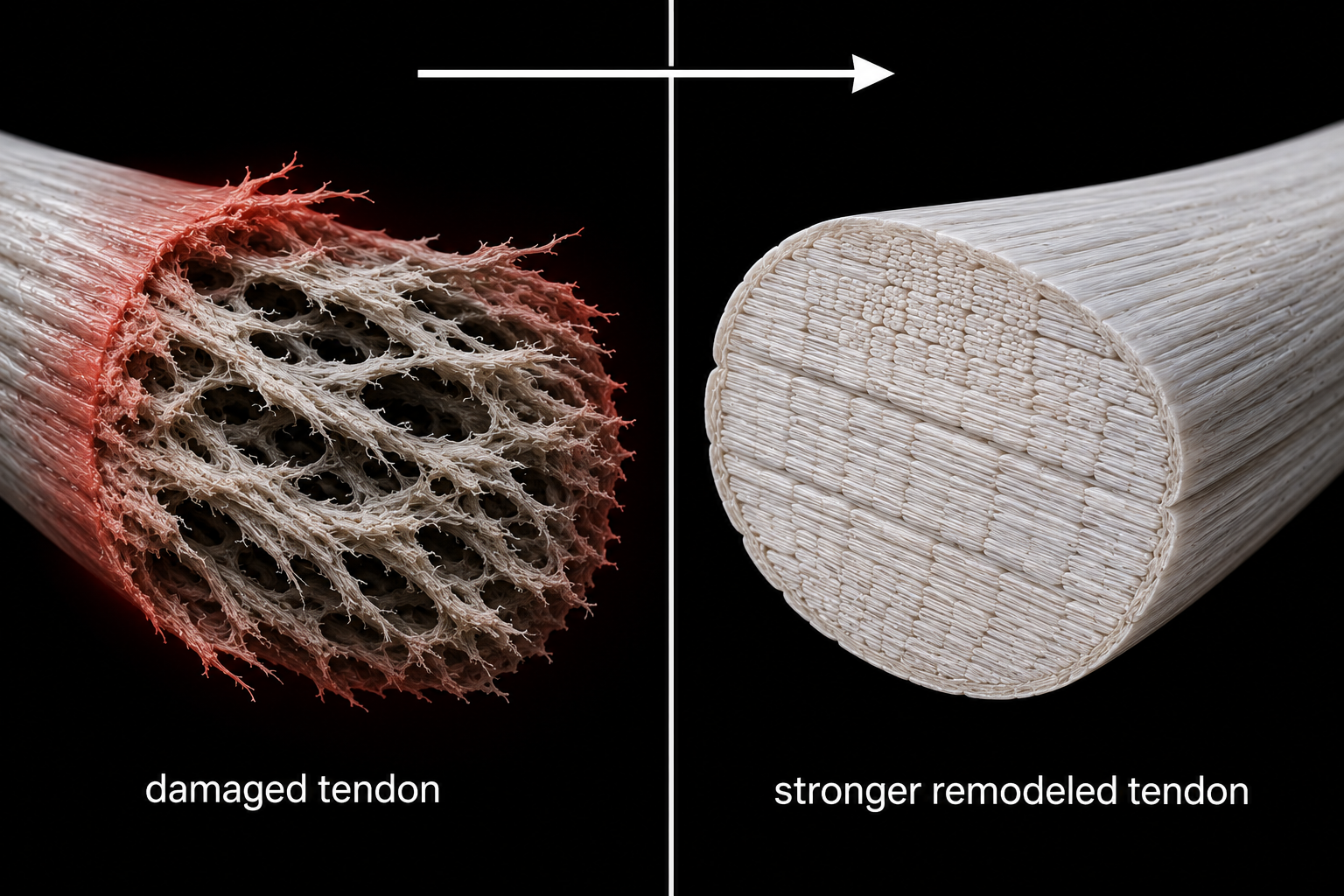
The anatomy of a tendon — organised collagen fibres transitioning into a disrupted, damaged region. Fast loading stress-shields this area. Slow isometric loading reaches it via stress relaxation.
1. Time: 30 Seconds
The contraction needs to last long enough for stress relaxation to develop meaningfully. The research points to 30 seconds as the effective minimum. At that duration, the tendon reduces its internal tension by approximately 45% — and this reduction in tension while under load is the signal the tissue reads as a stimulus to remodel and produce new collagen.
Five-second holds or ten-second holds don’t produce this response at any clinically relevant level. The duration is not a preference — it’s the mechanism.
2. Tension: Around 70% of Maximum Force Output
This is where most people underestimate the requirement. The load has to be high enough that it represents a genuine challenge to the tendon, not just the muscle. There needs to be sufficient mechanical demand on the connective tissue to register as a stimulus for structural change.
Research consistently identifies a loading threshold of around 70% of maximum force output. In practice — measured under force plates in a gym setting — this has meant 40–50 kg dumbbells for a split squat hold in some athletes, or over 90 kg loaded for a calf raise hold to generate sufficient force through the Achilles.
These are not gentle exercises. And this is precisely the point. A weak isometric contraction doesn’t give the tendon a reason to become stronger, for exactly the same reason that lifting very light weights gives your muscle no reason to grow. If you’ve been doing isometrics for tendon pain without results, insufficient load is almost certainly the missing variable.
3. Volume: Sets, Frequency, and the Pain Rule
The effective range is 3–6 sets per session, using 1–3 exercises. For maintenance or prehab on a healthy tendon, three sets of a single exercise done three times per week is sufficient. For active tendinopathy that has been persistent for months, working up to four to six sets across two or three exercises — and maintaining that consistently — is a more realistic target.
Frequency should be three times per week, or every other day. The reason is that net positive collagen synthesis occurs in the 24–36 hours following a loading session. Training daily doesn’t allow this cycle to complete. The recovery logic here is the same as for muscle: you can’t adapt during the session. You adapt in the window after it.
On pain: working through existing tendinopathy means some discomfort during loading is expected. Pushing to a 4 out of 10 on the pain scale during the exercise is acceptable — and evidence suggests it may actually accelerate remodeling compared to working completely pain-free. The key marker is what happens afterward: your pain should return to its baseline level within 24 hours of a session. If it doesn’t — if your overall pain level trends upward over several days — reduce volume or load before your next session.
Most people who've failed to resolve tendon pain for months weren't doing the wrong exercises — they were doing the right ones with insufficient load. The loading threshold has to be reached. A genuinely challenging 30-second isometric, three times a week, is not passive rehabilitation. It is progressive, targeted training for a tissue that responds to a very specific mechanical stimulus.
The Same Principle Works Anywhere in the Body
The mechanism above — sustained heavy loading creating stress relaxation in disrupted collagen — applies to every tendon in the body. The exercise changes; the protocol structure does not.
- Patellar tendinopathy (jumper’s knee): leg extension isometric, split squat isometric, leg press isometric
- Achilles tendinopathy: loaded calf raise hold with a barbell on your shoulders to generate sufficient force through the tendon
- Bicep tendon irritation: isometric front raise or an isometric bench press hold held at mid-range
- Hamstring tendons: long lever bridge holds, Nordic hamstring curl position hold
- Lateral elbow (tennis elbow): wrist extension isometrics, wrist supination isometrics
- Finger and wrist tendons: hangboard holds at appropriate finger pocket depth for those building toward climbing
In every case: 30-second holds, loaded to approximately 70% of your maximum effort for that exercise, 3–6 sets, three days per week.

The split squat isometric hold (left) and the leg extension isometric hold (right). Both are held for 30 seconds at a load that is genuinely challenging — not the lightest weight you can manage, but one that makes the hold difficult to complete.
Heavy Slow Resistance: The Alternative
Isometrics are the primary approach, particularly when managing active pain. But heavy slow resistance (HSR) training — full range-of-motion movement performed with deliberate slowness and heavy load — can produce comparable tendon adaptation.
The logic: a split squat performed at a 3-second descent and a 3-second ascent, under load heavy enough to make that genuinely difficult, creates a prolonged mechanical demand through the tendon at each point in the range. The tendon never fully unloads, and time under tension at each angle approximates the stimulus of an isometric hold.
The practical difference: isometrics are easier to control when pain is present, because you can select a specific joint angle that produces less discomfort and hold it precisely. HSR is a better fit for an off-season context where you want simultaneous tendon and muscle adaptation. If you use HSR, the principles remain the same — load it properly, use slow tempos, and respect the 48-hour recovery window between sessions.
A Note on Nutrition
The athletes in the case studies referenced above — both the NBA case and the Olympian — were using a specific supplementation protocol in conjunction with their loading sessions: 15 grams of gelatin combined with 225 mg of vitamin C, taken 30–60 minutes before each session.
The hypothesis is that pre-exercise collagen supplementation increases the availability of amino acid building blocks in circulation at exactly the moment the tendon is receiving the mechanical stimulus to produce new collagen. The evidence suggests this adds a small-to-moderate benefit to the rate of structural change compared to loading without it.
Supplementation is not required to see results. The loading protocol works without it. But if you’re working through a persistent tendinopathy and want to maximise the tissue response, the research does support including it.
This is not medical advice. Speak to a healthcare professional before adding any supplementation to your programme, particularly if you are managing an existing condition.
The Protocol at a Glance
| Variable | Target |
|---|---|
| Exercise type | Isometric hold (or heavy slow resistance) |
| Hold duration | 30 seconds |
| Load | ~70% of maximum force output |
| Sets per session | 3–6 |
| Exercises per session | 1–3 |
| Frequency | 3× per week / every other day |
| Acceptable pain during session | Up to 4/10 — must return to baseline within 24 hours |
| Optional pre-training nutrition | 15g gelatin + 225mg vitamin C, 30–60 min before |
Tendon damage was treated as a permanent condition for too long. The research over the past two decades tells a different story. The tissue is adaptable. The response is well-documented. And the protocol — specific, heavy, patient — is no more complicated than any other form of structured training.
If you’ve been managing tendon pain rather than addressing it, this is where to start.
Want help building a training system that accounts for tendons, joints, and long-term capacity — not just muscle?
Work With Us →